Understanding the Connection Between Hormones and Hair Loss
April 11, 2023
A symbol of femininity for so many women, our hair demands attention. Both deeply personal and superficially public, changes in the looks of our hair can inspire a range of emotions, driving us to willingly partake in its cutting, straightening, curling, bleaching, darkening, or other aggressive chemical treatments. Hair is part of who we are and how we present ourselves to the world. This is why thinning hair is kind of a big deal – it can be a very frustrating topic for many women as there is no quick solution to getting more hair instantly.
Losing hair is utterly dreaded and distressing, and unfortunately something we all eventually come to face as we get older. As hair thins over the years and the shower drain clogs almost on a daily basis, the scalp becomes so vivid when hair is a dash too oily, and now the hair part has been moved over to a different spot, thereby concealing the thinned out patches next to the temples – you find yourself on the internet in search of answers, bombarded with innumerable articles offering anywhere between 3 and 33+ helpful tips on how to get your luscious mane back. Some are obvious – eat right and exercise to provide nutrients and stimulate blood flow, while others are less straightforward like sleeping on a silk pillowcase or wrapping your hair in a T-shirt. Whatever the suggestions may be, achieving strong and healthy hair extends way beyond keeping your locks away from heat and dyes.
Ironically the phrase “beauty is only skin deep” is not entirely appropriate in conversations about hair. Thinning, dry hair is actually a symptom of internal changes in the body. Perhaps viewed by some as a normal, inevitable sign of aging or response to stress, losing hair is oftentimes related to endocrine imbalances. This blog is going to review the role that hormones play in hair health.
Hair Follicles Cycle Between Rest and Growth
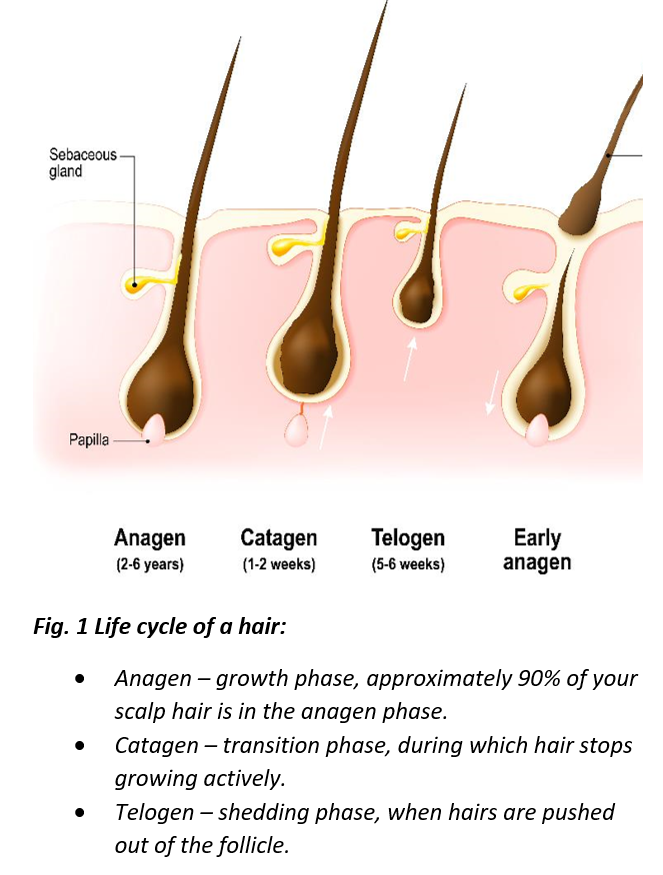
Before we jump into endocrine logistics, let’s review some anatomical considerations. Hair changes can occur due to alterations of the hair fiber itself, the hair cycle, and/or the hair follicle – the portion of hair beneath the surface of the skin. This human hair follicle is an intriguing structure! Hair follicles are incredibly productive, constantly undergoing cyclical rounds of rest (telogen), regeneration (anagen) and degeneration (catagen), and they are unique in this ability to dynamically alternate between rest and active growth.
The Stress - Tress Connection
We all know that stress is bad for you, including your hair. Bluntly speaking, stress makes your hair fall out. This is largely because stress puts you in survival mode, diverting resources away from good skin blood flow, adequate digestion, sleep, growth, etc. so the energy can be used instead for fight or flight. And let’s be honest, your body doesn’t regard hair as being essential to your survival.
Stress molecules like cortisol can target and damage the hair follicle [1]. You don’t even have to wait till menopause for stress-induced pony tail circumference shrinkage – many women in their 20s and 30s start losing hair due to stress-related issues [2].
Symptoms of sudden bouts of hair shedding with little to no hair growth are suggestive of telogen effluvium – a condition where hair in the anagen (growing) phase prematurely enters the telogen (resting) phase (Fig. 1) [3]. Furthermore, stress resulting from the hair loss itself (which for many people carries a significant psychological burden) aggravates and perpetuates the vicious cause-and-effect cycle that is doomed to keep repeating itself like “Groundhog Day”.
So take a moment to assess your stress burden and try to incorporate stress-reduction strategies in your daily life. For laboratory measures, diurnal cortisol testing in saliva or urine can help understand underlying biochemistry.
Sex Hormones – Not Just for Reproduction
PREGNANCY: Remember all that hair that you didn’t lose when you were pregnant? I loved my luxurious pregnancy hair – so strong, thick and shiny. It wasn’t me who had the “pregnancy glow”, it was my hair! Pregnancy increases the number of hair follicles in the anagen (translation: massive growth) phase. The enhanced supply of estradiol and progesterone in pregnancy are particularly nurturing to hair, expanding the growth phase and preventing shedding. Little did I know that at about 3 months postpartum, when my hormones were trying to re-equilibrate themselves and adjust to a “new normal”, my hair would all come out in clumps, washing down the drain, falling out so fast it was a seeming miracle any of it actually remained attached to my head.
Hair changes in pregnancy are common; however, every woman is different and therefore hair changes are all individual. If hair loss is experienced in the postpartum period, most women will experience a full recovery, although the process may be slow.
MENOPAUSE: Along those lines, when the levels of estradiol and progesterone fall in menopause, hot flashes and night sweats are not the only symptoms that seemingly appear out of nowhere. What many women are unaware of and unprepared for is the fact that they may also find themselves facing hair thinning. And just like the postpartum hair loss, it has everything to do with hormones. However, unlike the postpartum period, hair loss in menopause is irreversible, unless hormone replacement therapy is introduced.
|
Estrogen increases the amount of time that hair spends in the growing phase, so when estrogen declines, hair loses these protective effects. |
Estrogen increases the amount of time that hair spends in the growing phase, so when estrogen declines, hair (and skin, brain, heart, bones and many other tissues!) loses these protective effects. Additionally, androgenic effects of testosterone can also be intensified – where testosterone’s metabolite dihydrotestosterone (DHT) can produce progressively weaker hair due to the follicle’s failure to thrive [4]. When menopausal symptoms are present, a simple-to-collect saliva test can assess the levels of estradiol, progesterone, and testosterone, and help both patient and practitioner decide on the best therapeutic strategy.
PCOS: This is a common female endocrine disorder based on a cluster of symptoms, with hyperandrogenism taking center stage [5]. In PCOS, the “Alice in Wonderland” equivalent reality of elevated androgens, women lose scalp hair, while simultaneously growing hair in places where men usually get it and where women certainly don’t want it – face, chest and back. Although there is no cure for PCOS, treatment is usually focused on managing symptoms. A laboratory workup is typically performed for saliva steroids and blood levels of HbA1c and fasting insulin.
Ferritin – Not That Kind of Store
If you think of iron as the merchandise in the front of the store, ferritin is the storage warehouse in the back. Serum ferritin is a powerful screening tool for iron deficiency. Low serum ferritin gives rise to a condition called anemia.
For those of us who’ve been anemic at one point or another (thanks, heavy periods), we are all too familiar with the symptoms of being really tired and pale. While hair loss is not the most common symptom of iron-deficiency anemia, it does affect approximately half of those with low ferritin stores [6]. Hair follicles actually hang on to ferritin. When the body is low in iron, it can pull ferritin from places like hair follicles, deemed not as important as, let’s say, red blood cell production. The resulting effect is diffuse hair loss.
If hair loss is related to insufficient iron in the body, correcting anemia should allow for hair to grow back. But first, screening for low serum ferritin levels is very important, because supplementing with iron when iron levels are normal or high can result in iron overload and toxicity [7].
Thyroid Hormone
Thyroid hormone regulates pretty much every process in our body. When the thyroid system becomes underactive, like with hypothyroidism for example, our metabolism slows down, and the lesser important body functions get less attention. Sadly, hair (and skin) typically suffer first [8]. In hypothyroidism, hair tends to be dry, brittle, dull, and diffusely thinned out – even eyebrow hair can fall out [9]! When the reverse is true and there’s too much thyroid hormone (Graves’ disease), hair will also fall out.
Accompanying symptoms of thyroid disease are noticeably in energy levels and mood. Hypothyroidism tends to make people feel tired, sluggish, depressed, and constipated. Hyperthyroidism can manifest in anxiety, problems sleeping, restlessness, and irritability. If symptoms are present, check your thyroid levels and talk to your doctor about thyroid hormone therapy. In most cases, hair grows back once thyroid abnormalities are treated.
Vitamin D – the “Sunshine” Vitamin and so Much More!
Vitamin D is an important nutrient that is essential to our immunity, bone health and many other processes. With regard to hair, it actually helps create new hair follicles by initiating the anagen phase. It does so by regulating the expression of genes that are required for hair follicle cycling. A number of symptoms, such as hair loss, can occur when the body lacks enough vitamin D. It’s not surprising then when researchers found suboptimal serum vitamin D levels in women with telogen effluvium or female pattern hair loss [10]. Moreover, patients with alopecia areata, an autoimmune condition which gives rise to hair loss, also have low serum vitamin D levels [11]. Emerging clinical research is putting forward recommendations to evaluate serum vitamin D levels in patients with hair loss [12].
Most people can get the bulk of their vitamin D through sunlight exposure or through diet. Some foods are naturally rich in this nutrient, such as fatty fish (salmon, mackerel), mushrooms, or foods fortified with vitamin D (certain cereals and milk). Vegan or vegetarian diets tend to provide less vitamin D, so supplements may be needed. Additionally, finding a balance between protecting skin from sun exposure and absorbing the vitamin may be essential to achieving optimal vitamin D levels.
Vitamin B12 – the “Energy Vitamin”
To keep hair follicles active, you need healthy blood flow – the oxygen-rich red blood cells feed the hair follicles. Vitamin B12, also known as cobalamin, does exactly that – it promotes healthy hair growth by assisting in the production of these red blood cells.
Vitamin B12 is nicknamed “the energy vitamin”, and it makes sense that its deficiency can manifest as weakness and fatigue – symptoms that appear to overlap with other types of deficiencies described in this blog. If you're worried you may be deficient, a serum vitamin B12 test can rule out abnormalities. B12 deficiency is usually more prominent in folks with digestive issues (low stomach acid, gastritis, or celiac disease), in older adults, vegans, vegetarians, and with excessive alcohol intake. Vitamin B12 is found in animal-sourced foods such as meat and dairy, and in some fermented veggies. Plants don’t make vitamin B12, but during the fermentation process, certain types of bacteria can supply some of this nutrient.
Clinical Evaluation – Talk to Your Doctor!
A laboratory workup for hair loss is commonly performed. Additional questions that you may be asked to help narrow down differential diagnosis are [13]:
- When did the hair loss start? A sudden onset of hair loss may be suggestive of a disruption of the hair cycle.
- Where is the hair loss most prominent? Hair loss can be patchy, diffuse or patterned. Diffuse shedding may indicate disruption of the hair cycle, while patterned thinning could be attributed to hormonal dysregulation.
- What is the normal hair care routine? Certain hair care practices can have a tremendous impact on the loss of hair health.
With proper evaluation and appropriate testing for hormonal imbalances or nutritional deficiencies, help is on the way!
References
[1] Shin, H., et al., Acute Stress-Induced Changes in Follicular Dermal Papilla Cells and Mobilization of Mast Cells: Implications for Hair Growth. Ann Dermatol, 2016. 28(5): p. 600-606.
[2] Dinh, Q.Q. and R. Sinclair, Female pattern hair loss: current treatment concepts. Clin Interv Aging, 2007. 2(2): p. 189-99.
[3] Thom, E., Stress and the Hair Growth Cycle: Cortisol-Induced Hair Growth Disruption. J Drugs Dermatol, 2016. 15(8): p. 1001-4.
[4] Ramos, P.M. and H.A. Miot, Female Pattern Hair Loss: a clinical and pathophysiological review. An Bras Dermatol, 2015. 90(4): p. 529-43.
[5] Gersh, F., PCOS SOS. A Gynecologist's Lifeline To Naturally Restore Your Rhythms, Hormones, and Happiness. 2018: Integrative Medical Group of Irvine.
[6] Deloche, C., et al., Low iron stores: a risk factor for excessive hair loss in non-menopausal women. Eur J Dermatol, 2007. 17(6): p. 507-12.
[7] Trost, L.B., W.F. Bergfeld, and E. Calogeras, The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J Am Acad Dermatol, 2006. 54(5): p. 824-44.
[8] Contreras-Jurado, C., et al., Thyroid hormone signaling controls hair follicle stem cell function. Mol Biol Cell, 2015. 26(7): p. 1263-72.
[9] van Beek, N., et al., Thyroid hormones directly alter human hair follicle functions: anagen prolongation and stimulation of both hair matrix keratinocyte proliferation and hair pigmentation. J Clin Endocrinol Metab, 2008. 93(11): p. 4381-8.
[10] Rasheed, H., et al., Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol, 2013. 26(2): p. 101-7.
[11] Lee, S., et al., Increased prevalence of vitamin D deficiency in patients with alopecia areata: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol, 2018. 32(7): p. 1214-1221.
[12] Banihashemi, M., et al., Serum Vitamin D3 Level in Patients with Female Pattern Hair Loss. Int J Trichology, 2016. 8(3): p. 116-20.
[13] Mirmirani, P., Managing hair loss in midlife women. Maturitas, 2013. 74(2): p. 119-22.